
 Within the past decade, ads for Red Light Therapy (RLT) devices have
exponentially appeared in the health, wellness and commercial markets-
drawing significant attention to their claims and challenging their
efficacy. As with all technologies, many variables are to be considered
as far as concluding on their proposed health benefits. Published
reports from clinical (valid) studies detailing the utility of RLT in
human health. Encouraging reviews indicate that there is a growing body of evidence for the use of RLT in traumatic brain injury (TBI) and neurodegenerative processes, including Stroke and Parkinson’s disease.
Within the past decade, ads for Red Light Therapy (RLT) devices have
exponentially appeared in the health, wellness and commercial markets-
drawing significant attention to their claims and challenging their
efficacy. As with all technologies, many variables are to be considered
as far as concluding on their proposed health benefits. Published
reports from clinical (valid) studies detailing the utility of RLT in
human health. Encouraging reviews indicate that there is a growing body of evidence for the use of RLT in traumatic brain injury (TBI) and neurodegenerative processes, including Stroke and Parkinson’s disease. 
HealthTech Report (Theralight 360) Part 1
 To assess this innovation, we must first understand the scientific basics of RLT and the metabolic effects which have been documented and the ranges of red light therapy. On the market, there are many names thrown around representing similar protocols, all carrying varied effects.
To assess this innovation, we must first understand the scientific basics of RLT and the metabolic effects which have been documented and the ranges of red light therapy. On the market, there are many names thrown around representing similar protocols, all carrying varied effects.
’Infrared’ refers to a type of light that is below the spectrum of visible light. The naked eye cannot see this type of light. Light is measured in wavelengths, and to further define infrared, there are near infrared (NIR) and far infrared (FIR) wavelengths. FIR is what is typically found in many of the devices sold to the general public like infrared blankets and saunas. (Although, saunas, combine heat with light so the effects of FIR are not comparable.) FIR offers some mild effects, but it doesn’t penetrate the body as much as NIR. As a result, most clinical research published to date is on visible red/NIR because these have been shown to be more effective.
Visible red light, just as the name states, is visible to the naked eye, unlike infrared. When studies on light therapy are published, the wavelength of the light is always defined, and that is a very important factor in choosing what type of device to use. Even with NIR, the exact wavelengths of the light need to be taken into consideration. NIR (wavelength 800-900 nm) and red (wavelength 600 nm) have been shown to penetrate through scalp and skull and have the potential to improve the subnormal, cellular activity of compromised brain tissue (1).

Wireless frequency controls (tablet)
Upon review (both historically and through firsthand observation) the function of the various red light waves have shown physiological effects and benefits on the body, and more specifically the brain. Well documented effects of red/NIR light include: anti-inflammatory, anti-apoptotic, antioxidant, and neurogenesis and synaptogenesis, which has led to numerous studies focused on the areas of cognitive decline, Alzheimer’s, Parkinson’s disease, stroke, traumatic brain injury, and various other brain and nervous system disorders.
TRAUMATIC BRAIN INJURY  In light of the current limited therapeutic options for TBI, the utility of red light therapy in clinical practice has offered many benefits. Functional magnetic resonance imaging has shown modulation of activation in intrinsic brain networks likely to be damaged in TBI (specifically, the default mode network and salience network). Furthermore, improvement in executive function, working memory, and sleep (chronic effects of TBI), have also been documented. RLT can help the brain repair itself by stimulating neurogenesis, upregulating BDNF synthesis, and encouraging synaptogenesis. (2)
In light of the current limited therapeutic options for TBI, the utility of red light therapy in clinical practice has offered many benefits. Functional magnetic resonance imaging has shown modulation of activation in intrinsic brain networks likely to be damaged in TBI (specifically, the default mode network and salience network). Furthermore, improvement in executive function, working memory, and sleep (chronic effects of TBI), have also been documented. RLT can help the brain repair itself by stimulating neurogenesis, upregulating BDNF synthesis, and encouraging synaptogenesis. (2)
To explore how treatment with RLT for TBI works in a clinical setting, a small preliminary study of eleven adult chronic TBI patients who suffered from persistent cognitive dysfunction were treated for 18 outpatient sessions of RLT (Monday, Wednesday, Friday, for 6 weeks) starting at 10 months to 8 years post-event, some with a history of multiple concussions. Subjectively, participants reported improved sleep, and fewer post-traumatic stress disorder (PTSD) symptoms, if present. Participants and family reported better ability to perform social, interpersonal, and occupational functions. Objective neuropsychological testing at 1 week, and 1 and 2 months after the 18th treatment showed significant linear trend improvement over time in the area of executive function. (3) Certainly, encouraging results seen here and reflective of what clinicians who use RLT observe in private practice.


’Infrared’ refers to a type of light that is below the spectrum of visible light. The naked eye cannot see this type of light. Light is measured in wavelengths, and to further define infrared, there are near infrared (NIR) and far infrared (FIR) wavelengths. FIR is what is typically found in many of the devices sold to the general public like infrared blankets and saunas. (Although, saunas, combine heat with light so the effects of FIR are not comparable.) FIR offers some mild effects, but it doesn’t penetrate the body as much as NIR. As a result, most clinical research published to date is on visible red/NIR because these have been shown to be more effective.
 |
| Wireless frequency controls (tablet) |

"GETTING BACK TO ACTIVE""I had severe sciatica pain making it painful to walk. it was caused by a herniated disc and spinal stenosis... After about a month of treatment (with the Theralight) a few days a week, my nerve pain was GONE! I could walk with absolutely no more pain. I can now participate in all of the activities I enjoyed prior to my nerve pain. I walk as much as I can- daily. Now, I can practice yoga daily. The Theralight along with Dr. Stagg's treatment has completely eliminated all my issues and get my life back!"- Kathy
 DR. JENNIFER STAGG is the medical director of Whole Health Wellness Center (CT). She is also the author of The Bitter Prescription and Unzip Your Genes and is routinely featured as an expert guest in the media on the topic of nutrigenomics and integrative medicine. Her areas of clinical expertise include mental health, weight loss resistance and nutrition, digestive health, metabolic and endocrine disorders, and nutrigenomics. (learn more about Dr. Stagg @ her professional website)
DR. JENNIFER STAGG is the medical director of Whole Health Wellness Center (CT). She is also the author of The Bitter Prescription and Unzip Your Genes and is routinely featured as an expert guest in the media on the topic of nutrigenomics and integrative medicine. Her areas of clinical expertise include mental health, weight loss resistance and nutrition, digestive health, metabolic and endocrine disorders, and nutrigenomics. (learn more about Dr. Stagg @ her professional website)
1. Dos Santos JGRP, Paiva WS, Teixeira MJ. Transcranial light-emitting diode therapy for neuropsychological improvement after traumatic brain injury: a new perspective for diffuse axonal lesion management. Med Devices (Auckl). 2018 Apr 26;11:139-146.2. Hamblin MR. Photobiomodulation for traumatic brain injury and stroke. J Neurosci Res. 2018 Apr;96(4):731-743. doi: 10.1002/jnr.24190. Epub 2017 Nov 13. Erratum in: J Neurosci Res. 2019 Mar;97(3):373.3. Naeser MA, Zafonte R, Krengel MH, Martin PI, Frazier J, Hamblin MR, Knight JA, Meehan WP 3rd, Baker EH. Significant improvements in cognitive performance post-transcranial, red/near-infrared light-emitting diode treatments in chronic, mild traumatic brain injury: open-protocol study. J Neurotrauma. 2014 Jun 1;31(11):1008-17Naturopathic Physician, Author, Speaker, Educator, Consultant

Photobiomodulation Research Accepted for Peer Reviewed PublicationsStudies Reveal Positive Outcomes Using Aspen Lasers for Treatment of Challenging Conditions
 LINDON, Utah, March 9, 2022 /PRNewswire/ -- Aspen Laser, LLC, an emerging global leader in the medical device industry, with a focus on photomedicine, announced that research involving Aspen Laser, a Class IV laser therapy device, has been peer reviewed, accepted, and recently published in three medical journals: Photobiomodulation, Photomedicine, and Laser Surgery Journal (Mary Ann Liebert, Inc.), OBM Integrative and Complementary Medicine Journal (LIDSEN Publishing Inc.), and The Journal of Lasers in Medical Sciences. Justin Vorwaller, MBA, COO of Aspen Laser stated, "We are pleased that recent research utilizing Aspen Laser technology is being published, providing new validation that is promoting the understanding and application of Photobiomodulation (PBM) further. This will also provide healthcare professionals a scientifically-based reason to integrate PBM into their practices, improving the quality of their patient's lives, including those where other treatments have failed, but are now proven in these studies." (See complete press release 3/2022)
LINDON, Utah, March 9, 2022 /PRNewswire/ -- Aspen Laser, LLC, an emerging global leader in the medical device industry, with a focus on photomedicine, announced that research involving Aspen Laser, a Class IV laser therapy device, has been peer reviewed, accepted, and recently published in three medical journals: Photobiomodulation, Photomedicine, and Laser Surgery Journal (Mary Ann Liebert, Inc.), OBM Integrative and Complementary Medicine Journal (LIDSEN Publishing Inc.), and The Journal of Lasers in Medical Sciences. Justin Vorwaller, MBA, COO of Aspen Laser stated, "We are pleased that recent research utilizing Aspen Laser technology is being published, providing new validation that is promoting the understanding and application of Photobiomodulation (PBM) further. This will also provide healthcare professionals a scientifically-based reason to integrate PBM into their practices, improving the quality of their patient's lives, including those where other treatments have failed, but are now proven in these studies." (See complete press release 3/2022)

 Photobiomodulation Research Accepted for Peer Reviewed Publications Studies Reveal Positive Outcomes Using Aspen Lasers for Treatment of Challenging Conditions  |
"Personalized medicine is an emerging practice of medicine that uses an individual's genetic profile to guide decisions made in regard to the prevention, diagnosis, and treatment of disease. Knowledge of a patient's genetic profile can help doctors select the proper medication or therapy and administer it using the proper dose or regimen. Personalized medicine is being advanced through data from the Human Genome Project." -NIH Originally published: March 2022
NEW HOPE FOR GENETIC DISEASESWritten by: Dr. Bobbi KlineOne of the biggest controversies in screening for inherited diseases with genetic testing is the lack of effective tools to help people feel empowered. People found to carry one of these genetic mutations that cause disease often felt like it was a death sentence. Even armed with the latest medications or surgeries, often they felt helpless, just waiting for the day when they got the bad news. Thankfully that conversation is changing with genomics and Personalized Medicine. When you understand the biology and biochemistry of our bodies – and the genes that run them, it is very clear that there is much more that can be done to alter the perceived fated outcome. But the scientific studies have lagged behind – until now.
 A recent study published in Nature (1) is providing support for the polygenic model of genomics. This model is an advanced application of Personalized Medicine utilizing genomics - the newer branch of genetics. Rather than the conventional single gene- single outcome model, this newer approach takes into account multiple genes involved in multiple biochemical pathways, and how small changes in these genes called single nucleotide polymorphisms (SNPs for short) each contribute to disease over time. [see: genetics vs genomics] It’s much more complicated, and as a result much harder to study. It’s also much harder to address with a single medication or the limited approach of conventional medicine.
A recent study published in Nature (1) is providing support for the polygenic model of genomics. This model is an advanced application of Personalized Medicine utilizing genomics - the newer branch of genetics. Rather than the conventional single gene- single outcome model, this newer approach takes into account multiple genes involved in multiple biochemical pathways, and how small changes in these genes called single nucleotide polymorphisms (SNPs for short) each contribute to disease over time. [see: genetics vs genomics] It’s much more complicated, and as a result much harder to study. It’s also much harder to address with a single medication or the limited approach of conventional medicine.But now that is changing. In this research study, they looked at 3 diseases with a strong genetic link: hereditary breast and ovarian cancer, familial hypercholesterolemia, and Lynch syndrome. They evaluated more than 80,000 individuals of primarily European ancestry to examine the interaction between SNPs in multiple genes in other systems (polygenic) and single gene (monogenic) mutations for these specific inherited diseases.
The study showed that there was a wide range of risk as to whether someone who carried one of these mutations actually developed the disease. The probability of disease by the age of 75 ranged from 17% to 78% for coronary artery disease; 13% to 76% for breast cancer; and 11% to 80% for colon cancer (Lynch syndrome). And the explanation was the influence of this polygenic model on the effect of the genetic mutation.
KNOWING YOUR BLUEPRINT & STRATEGIC INTERVENTIONWe can potentially modify the outcome of inherited diseases by understanding the multiple biochemical pathways and mechanisms involved, along with the genes that impact them. The key is in going beyond the conventional fated model of one gene-one disease, and integrating the more advanced polygenic model. This may make a difference as to what surveillance and intervention strategies are chosen for an individual. Perhaps equally or even more importantly, it opens up the opportunity to use a person’s genomic blueprint to be able to lower a person’s risk. By leveraging the function of these genes and their biological systems through targeted diet, lifestyle, supplement and even perhaps medication strategies, we can potentially alter the course of what was once thought to be an inevitable outcome.
Now we have the start of what promised to completely change how we approach genetic diseases, and what those of us practicing Personalized Medicine have been seeing for years in our practices - certain genetic mutations may not leave us as helpless as we thought. While there is still much scientific study that needs to be done, we have the tools and the power right now to make a difference.
References: Fahed, A.C., Wang, M., Homburger, J.R. et al. Polygenic background modifies penetrance of monogenic variants for tier 1 genomic conditions. Nat Commun 11, 3635 (2020). https://doi.org/10.1038/s41467-020-17374-3
Originally published: March 2022
Thankfully that conversation is changing with genomics and Personalized Medicine. When you understand the biology and biochemistry of our bodies – and the genes that run them, it is very clear that there is much more that can be done to alter the perceived fated outcome. But the scientific studies have lagged behind – until now.
A recent study published in Nature (1) is providing support for the polygenic model of genomics. This model is an advanced application of Personalized Medicine utilizing genomics - the newer branch of genetics. Rather than the conventional single gene- single outcome model, this newer approach takes into account multiple genes involved in multiple biochemical pathways, and how small changes in these genes called single nucleotide polymorphisms (SNPs for short) each contribute to disease over time. [see: genetics vs genomics] It’s much more complicated, and as a result much harder to study. It’s also much harder to address with a single medication or the limited approach of conventional medicine.But now that is changing. In this research study, they looked at 3 diseases with a strong genetic link: hereditary breast and ovarian cancer, familial hypercholesterolemia, and Lynch syndrome. They evaluated more than 80,000 individuals of primarily European ancestry to examine the interaction between SNPs in multiple genes in other systems (polygenic) and single gene (monogenic) mutations for these specific inherited diseases.
The study showed that there was a wide range of risk as to whether someone who carried one of these mutations actually developed the disease. The probability of disease by the age of 75 ranged from 17% to 78% for coronary artery disease; 13% to 76% for breast cancer; and 11% to 80% for colon cancer (Lynch syndrome). And the explanation was the influence of this polygenic model on the effect of the genetic mutation.
This may make a difference as to what surveillance and intervention strategies are chosen for an individual. Perhaps equally or even more importantly, it opens up the opportunity to use a person’s genomic blueprint to be able to lower a person’s risk. By leveraging the function of these genes and their biological systems through targeted diet, lifestyle, supplement and even perhaps medication strategies, we can potentially alter the course of what was once thought to be an inevitable outcome.
Now we have the start of what promised to completely change how we approach genetic diseases, and what those of us practicing Personalized Medicine have been seeing for years in our practices - certain genetic mutations may not leave us as helpless as we thought. While there is still much scientific study that needs to be done, we have the tools and the power right now to make a difference.
References: Fahed, A.C., Wang, M., Homburger, J.R. et al. Polygenic background modifies penetrance of monogenic variants for tier 1 genomic conditions. Nat Commun 11, 3635 (2020). https://doi.org/10.1038/s41467-020-17374-3
MODERN HEALTH STRATEGY: INTEGRATIVE MODALITIES By: Dr. Jonathan Kirschner, Physiatrist- Hospital for Special Surgery, NYC  (See Dr. Kirschner's complete feature article on the 2022 LIFE EXTENSION REVIEW at Health & healing 101) |
How to Choose the RIGHT DOCTOREdited by: Noelle Cutter, PhD

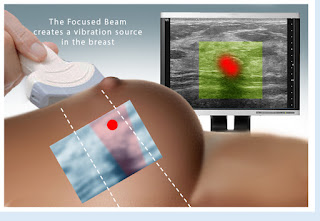
Power Doppler Sonography adds increased accuracy to breast imaging evaluation over ordinary ultrasound because it shows higher blood flow speeds, often a sign of cancerous activity in the breast. Studies have shown that suspicious blood flow identified by pre-surgery Power Doppler scans corresponds very well with the size, location and aggression of actual tumors that are then surgically removed. Thus, Power Doppler brings an important clinical dimension to breast cancer detection. 3D sonography clearly shows tumor margins and 3D Doppler affords an index of cancer aggression and metastatic potential.
Breast Sonograms and Ultrasound offers the following advantages:
• Highest accuracy in dense (lumpy, cystic) breasts
• Non-invasive-no radiation exposure
• Cost effective
• Can distinguish cysts (fluid-filled masses) from cancerous tumors without needle sampling
• Ease of image guidance for breast biopsy
Women who should consider ultrasound scanning of the breast include those at risk of breast cancer because of personal or family history and the presence of fibrocystic (dense) breast tissue which increases cancer risk by as much as 400%. (See complete program- LINK)
WHY CANCER COMES BACK (Source: NIH- National Cancer Institute) When cancer comes back after treatment, doctors call it a recurrence- or recurrent cancer. Finding out that cancer has come back can cause feelings of shock, anger, sadness, and fear. But you have something now that you didn’t have before—experience. You’ve lived through cancer already and you know what to expect. Also, remember that treatments may have improved since you were first diagnosed. New drugs or methods may help with your treatment or in managing side effects. In some cases, improved treatments have helped turn cancer into a chronic disease that people can manage for many years.Recurrent cancer starts with cancer cells that the first treatment didn’t fully remove or destroy. This doesn’t mean that the treatment you received was wrong. It just means that a small number of cancer cells survived the treatment and were too small to show up in follow-up tests. Over time, these cells grew into tumors or cancer that your doctor can now detect.
Recurrent cancer starts with cancer cells that the first treatment didn’t fully remove or destroy. This doesn’t mean that the treatment you received was wrong. It just means that a small number of cancer cells survived the treatment and were too small to show up in follow-up tests. Over time, these cells grew into tumors or cancer that your doctor can now detect.





No comments:
Post a Comment